67 Woman Abdominal Distention Vomited Three Times Continued to Pass Flaturs Nbme 4
April 17, 2021

Abdominal bloating and distension are two of the most commonly reported gastrointestinal symptoms, affecting people diagnosed with a broad range of underlying medical and surgical disorders. Nearly 40% of the general population reports having problems with these symptoms, and that rate is even higher among people diagnosed with other functional gastrointestinal disorders, including functional dyspepsia, irritable bowel syndrome (IBS) and functional constipation. Individuals with chronic and moderate to severe symptoms report that these symptoms negatively impact their activity level and quality of life.
In a narrative review published in Clinical Gastroenterology and Hepatology in 2021, co-authors Brian E. Lacy, M.D., Ph.D., David J. Cangemi, M.D., and Maria I. Vazquez-Roque, M.D., review the epidemiology, effects and pathophysiology of chronic bloating and distension and discuss diagnostic strategies and available treatment options. Drs. Lacy, Cangemi and Vazquez-Roque are gastroenterologists at Mayo Clinic's campus in Jacksonville, Florida.
Pathophysiology
Abdominal bloating and distension have a complex etiology that is not well understood. The list of possible causes includes organic, pathological conditions, disorders of gut-brain interaction and an abnormal viscerosomatic reflex.
Organic causes
The two most common causes within this category are small intestinal bacterial overgrowth (SIBO) and intolerance to carbohydrates and other food groups. Both conditions can prompt excess growth of bacteria, carbohydrate fermentation and, subsequently, gas production that causes the intestinal tract to stretch and distend. Recent research estimates that nearly 20% of the general population experiences some form of food intolerance.
The list of organic disorders that can cause bloating and distension also includes celiac disease, pancreatic insufficiency, prior gastroesophageal surgery (such as fundoplication or bariatric procedures), gastric outlet obstruction, gastroparesis, ascites, gastrointestinal or gynecologic malignancy, hypothyroidism, adiposity, small intestine diverticulosis, and chronic intestinal pseudo-obstruction.
Functional causes
Gut-brain interaction disorders associated with bloating and distension include IBS, chronic idiopathic constipation, pelvic floor dysfunction, functional dyspepsia and functional bloating. According to Drs. Lacy and co-authors, some individuals with these diagnoses have a visceral sensory disorder that causes them to perceive that their bodies are producing an excessive amount of gas.
"Many of these patients with visceral hypersensitivity actually produce normal amounts of gas, and the problem lies with their perception of the sensations that accompany that process," says Dr. Lacy. "These are frequently patients who have other sensory disorders, such as IBS, migraines, chronic fatigue or fibromyalgia."
These patients can have a conscious perception of intraluminal content and abdominal distension that may contribute to symptomatic bloating. "Complex brain-gut neural pathways, amplified by factors such as anxiety, depression, somatization and hypervigilance can also contribute to this perception of bloating," adds Dr. Lacy.
Abnormal viscerosomatic reflex
Bloating and distension can also be triggered by an abnormal viscerosomatic reflex. This reflex controls gas clearance and involves the contraction and relaxation of diaphragm and abdominal wall muscles. In individuals who have an abnormal response to a normal release of intestinal gas, the diaphragm descends or contracts inappropriately, and the abdominal wall muscles relax, allowing the abdomen to protrude.
Diagnostic strategies
Determining the etiology of abdominal bloating and distension can be challenging. For this reason, Dr. Lacy advises that acting like "good detectives" can help clinicians make an accurate diagnosis. Conducting a thorough clinical history and physical examination that includes the following details will help determine which type of testing may be needed:
- Onset and timing of symptoms
- Relationship to diet
- Use of medications and supplements
- Surgical history
- Bowel movement habits and patterns
"Asking about diet and thinking about bacterial overgrowth, visceral hypersensitivity, bowel disorders such as constipation and IBS, and whether these symptoms are related to an abnormal viscerosomatic reflex is part of the process," says Dr. Lacy.
Testing should be based on suspected etiology and can include:
- Breath tests, a widely available, inexpensive and noninvasive way to determine whether SIBO or food intolerance is responsible
- Upper endoscopy for patients with alarm symptoms (recurrent nausea and vomiting, unexplained anemia, hematemesis, 10% weight loss, or a family history of gastroesophageal malignancy) or when gastric outlet obstruction, gastroparesis or FD is suspected
- Celiac serologies to help determine if malabsorption of wheat and gluten is occurring
- Abdominal imaging, including computerized tomography or magnetic resonance imaging enterography for patients with constipation, prior abdominal surgery, Crohn's disease, or known or suspected small bowel dysmotility
- Complete gastrointestinal transit assessment, using scintigraphy or a wireless motility capsule, to confirm dysmotility or constipation secondary to slow transit
- Anorectal manometry with balloon expulsion for evaluation of anorectal disorders
Developing a management strategy
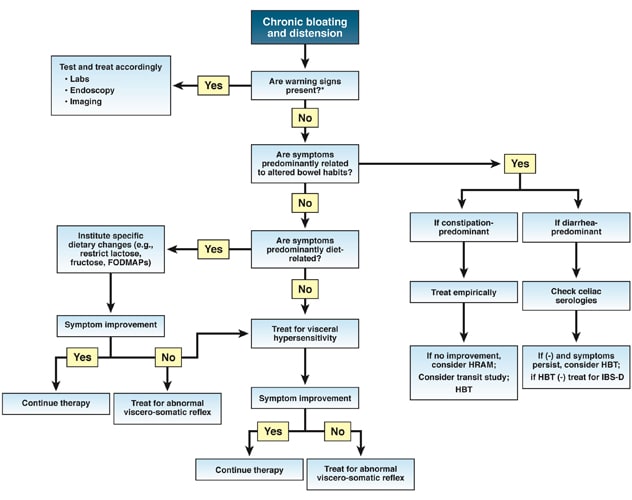
Given the broad range of possible causes associated with bloating and distension, identifying the most effective treatment for each individual with symptoms can be a complex process. Therapeutic options include dietary changes, probiotics, antibiotics, prokinetic agents, antispasmodics, neuromodulators and biofeedback. According to Dr. Lacy and co-authors, more than one treatment strategy may be necessary. The chronic bloating and distension treatment algorithm outlines a process for managing patients with these symptoms.
For more information
Lacy BE et al. Management of chronic abdominal distension and bloating. Clinical Gastroenterology and Hepatology. 2021;19:219.
Source: https://www.mayoclinic.org/medical-professionals/digestive-diseases/news/understanding-and-managing-chronic-abdominal-bloating-and-distension/mac-20511032
0 Response to "67 Woman Abdominal Distention Vomited Three Times Continued to Pass Flaturs Nbme 4"
Post a Comment